Interview with Prof. Pekka Vallittu, Finland 
Could you please shortly introduce yourself?
Professionally, I started as a dental technician and later became a dentist as well. During my undergraduate course, from 1988, I already started with research on the use of several types of fibres to reinforce dentures. In 1994, I completed my doctoral dissertation on this topic. Shortly thereafter, I stayed for almost two years at the Nordic Institute of Dental Materials where I had the chance to do research with Dr I. E. Ruyter, one of the most renowned experts in polymer chemistry for dental applications.
Here, I gained deep knowledge on that topic. Then, I returned to the University of Turku and I was one of the founders of Stick Tech (spin-off of the University of Turku, red.) in 1997. However, I made the personal decision to stay at the university rather than proceeding in the company, where I got governmental funding to continue research on fibre-reinforced composite. Through these many years of research, we had the chance to build a substantial amount of evidence and expertise in fibrereinforced composites. In 2006 I became Professor and Chair of the Department of Biomaterials Science and in 2009, director of the Turku Clinical Biomaterials Centre (TCBC). I’ve been the Dean of the Institute of Dentistry of the University of Turku from 2004 to 2012 and after a short break, returned to that position in 2018.
In your opinion, what are the main advantages of fibres in dentistry?
Fibres are the only way to make large direct restorations with good mechanical properties and durability. Other durable strong materials, such as zirconia and metal can only be made indirectly, outside the mouth. This way we can provide more affordable restorations and allow a larger patient group to be treated. Another advantage is that the mechanical properties of fibre- reinforced composites are very close to those of bone and dentine, which is not the case with metals or ceramics, which are very rigid. Fibre-reinforced composites are the only synthetic materials which meet the same biomechanical demands as dentine or bone.
What was the purpose of developing everX Flow?
Research started with long fibres, used in the everStick products, which are the most durable ones. However, length is also a matter of designation, and appliances and restorations like splints and bridges that cover a wide span need a different length compared to a single tooth restoration. The main purpose with which we started the development of everX Posterior was to find the optimal fibre length vs. the size of the tooth, so that the fibres would act as reinforcement. This resulted in an average fibre length of 0.7 mm to 1 mm in everX Posterior, which provided excellent mechanical properties, and in particular, increased toughness. However, the adaptation and placement were not always as easy to achieve as we ideally would like to. Meanwhile, the bulk-fill composites emerged onto the dental markets and became popular, not because of their properties but because of their ease of use. Hence, the idea arose to develop a flowable version.
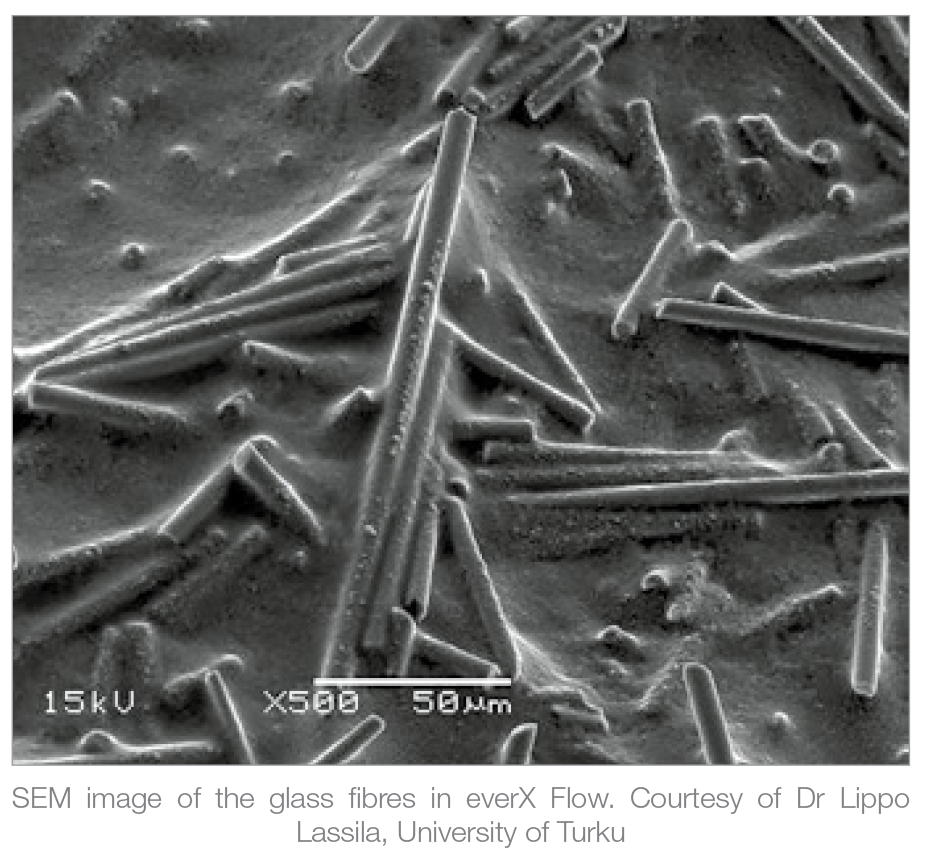
On one hand, we expected that shortening the fibres would decrease the properties. But, from studying the literature, we knew that the fibre length should be proportional to the diameter. Thus we started searching for what is called the ‘Optimal Aspect Ratio’. The fibres in everX Flow are shorter, but also thinner. With these smaller fibres, the viscosity could be changed; the fibres in everX Flow are about 0.1 mm in length but with a much smaller diameter. The amount of fibres could also be increased, maintaining the toughness – which is the main purpose of the fibre reinforcement. Most of the research is focused on the toughness because it has been shown to be the best indicator of longevity of a restoration. 1
What was your role in the development of this material?
I have initiated and coordinated the development of FRC materials. The key lab research has been mainly executed by Dr. Lippo Lassila who is the principal investigator in this particular project with Adjunct Professor Sufyan Garoushi and our skilled laboratory staff members. Dr. Garoushi wrote a PhD thesis on short fibre-reinforced composites. Further on, I have participated in the clinical test phase and directed the project form the clinical and material science perspectives. The entire project was a cooperation in which TCBC was in charge of the research and development of the research and Stick Tech – now a member of the GC group – transformed the research into an industrial project.
You often refer to fibre- reinforced composites as biomimetic restorations. What exactly do you mean with this term?
When you analyse human tissue, dentine and bone are fibre-reinforced materials, based on collagen fibres and apatite minerals. Even though the chemical composition of fibre- reinforced composites is different, they reproduce a similar structure. Moreover, the biomechanical behaviour of these composites mimics that of dentine.
Are there other differences between everX Posterior & everX Flow? Do they have the same indications?
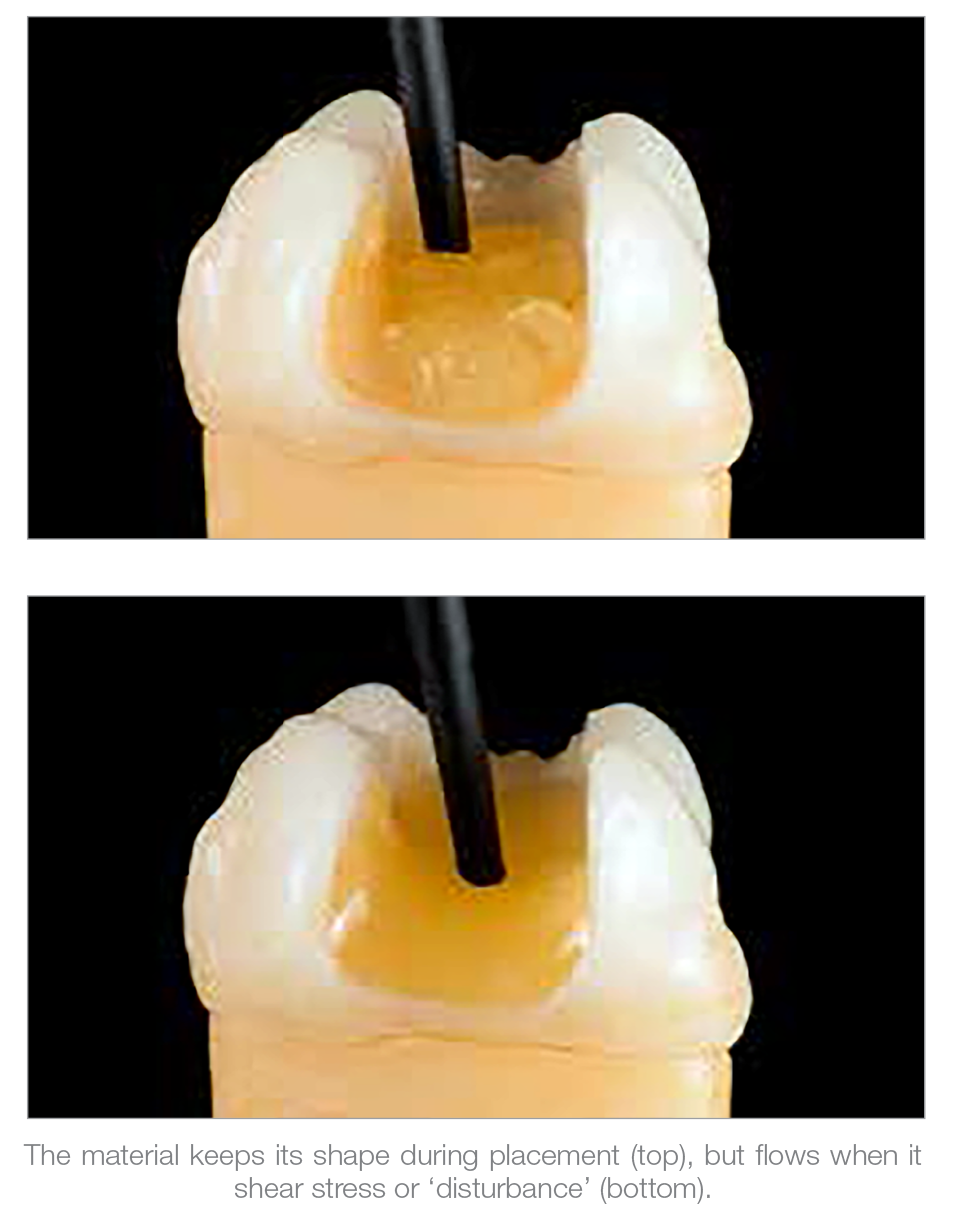
The indications are very similar, but the main difference is in the handling, because of the viscosity. Basically, they are both base materials to reinforce restored teeth. everX Flow is now also indicated as a core build-up material for metal and ceramic crowns.
There are 2 shades available in everX Flow. What are the differences & when are they indicated?
The ‘Bulk’ shade: is more translucent and can be cured in layers up to 5.5 mm, which widens the indications a bit. The ‘Dentin’ shade is more aesthetic and can be cured up to 2.0 mm.
What is the difference between traditional bulkfill composites and everX Flow?
In indications, they are very close to each other. However, everX Flow is a base material, meant to reinforce the structures underneath and above it. It needs to be covered with a regular composite that can be easily polished. Even though many bulk-fill composites need to be covered as well, in its strict definition, it should mean that you can use one and the same material from the bottom to the surface, in one increment.
How much stronger is everX Flow? What is the impact on performance?
Its toughness, which the most important material property impacting the clinical success1 is twice as much as any other kind of composite on the market, which is also the case for everX Posterior. Its impact on the restoration performance depends on the size and shape of the destructed tooth and the ratio of everX Flow and overlaying composite. The ratio between the short-fibre reinforced base and conventional composite in the restoration should be analogue to the dentine and enamel structure. This means that about 1-1.5 mm of the occlusal surface should be regular composite in order to give the best mechanical strength for the restored tooth as a whole2-3. Less benefit is achieved if the layer of fibrereinforced composite is not sufficiently thick4.
As a rule of thumb, you use everX Flow to replace dentine and regular composite to replace enamel, thus mimicking tooth structure.
Do you need to cover everX Flow with a last layer of composite, and if yes why?
By structure, everX Flow contains both micro and macrofill particles. Fibres are big particles that make it slightly less polishable even though the wear resistance in vitro is very good. Based on the wear behaviour, it could be exposed in approximal contact points. However, the official instruction remains to cover everX Flow on the proximal surfaces with regular composite as well.
More research is needed to analyse the effect in the long term, but available data are positive.
What does the research say about the performance of the product?
There is already a large number of publications available on everX Flow. On everX Posterior, we have even more evidence available. Almost all studies show superior properties of the material, such as the toughness or other mechanical properties. In vitro, it has been shown that fracture propagation is prevented in a restoration with fibre-reinforced composite. This is also the case at the interface of composite layers5.
In those studies where no considerable reinforcing effect was found, the thickness of the fibre-reinforced layer was usually insufficient. Studies from other research groups have confirmed these superior mechanical properties and there are still many studies ongoing on this topic.
Could everX Flow be used to replace posts? If yes, in which indications?
At the TCBC, we have been looking in this topic a lot, in vitro as well as clinically, and many other research groups are doing so as well. Overall, more research on this topic is still necessary. In molars, it is possible to make a direct endocrown without post by making a base of everX Posterior and this can be extrapolated to everX Flow as well.
This type of endocrown is analogue to lab-made ceramic endocrowns. The restoration only extends about 2-3 mm into the root canals, given that the walls are parallel and diameter is sufficient. The intraradicular part of the restoration should have the same height or be higher than the coronal part. The thickness of the occlusal veneer of the restoration should be more than 1-2 mm.
In anterior and premolars, studies have been done with very promising, but there is not enough evidence yet for clinical recommendation. However, it is possible to combine the pre-fabricated fibre post and use everX Flow in the coronal part of canal to replace cement and for the core.
This is an improvement in comparison with a regular luting cement.
Of course, results depend a lot on the remaining tooth structure. If there is considerable damage up to the gingival level a thick and well bonded fibre post is still needed for sufficient retention. Evidence might be available within 2-3 years.
What are your future research topics?
Tomorrow I’ll be giving a lecture on the masticatory function of giant pandas and the evolutionary adaptation of the condyles to that function. In the field of fibre-reinforced composites, we strive to an even closer resemblance to natural dentine; among others we are investigating nanofibres, and compositions and structure closer to apatite minerals. We are also cooperating with another research group to extended indications in surgical applications, taking into consideration the biological aspect of bone forming cell lines. This is linked also to the bone regeneration materials used in periodontology and oral surgery.
Article Published June - Aug 2024 Dental Solutions
References
1. Heintze SD, Hickel R, Reis A, Loguercio AS, Rousson V, Dent Mater 2017;33:e101-e114.
2. Omran TA, Garoushi S, Lassila L, Shinya A, Vallittu PK. Bonding interface affects the load-bearing capacity of bilayered composite. Dent Mater J. 2019; 38(6):1002-1011.
3. Garoushi S, Lassila LV, Tezvergil A, Vallittu PK. Load bearing capacity of fibre-reinforced and particulate filler composite resin combination. J Dent 2006; 34:763-769.
4. Rocca GT, Saratti CM, Poncet A, Feilzer AJ, Krejci I. The influence of FRCs reinforcement on marginal adaptation of CAD/CAM composite resin endocrowns after simulated fatigue loading. Odontology 2016; 104:220-232.
5. Tiu J, Belli R, Lohbauer U. Rising R-curves in particulate/ fiber-reinforced resin composite layered systems. J Mech Behav Biomed Mater. 2019;103:103537.