
Introduction
For dental practitioners and their patients, latex exposure can cause allergic reactions ranging from contact dermatitis to life-threatening anaphylaxis.
An unprecedented rise of latex allergy in dental and medical health care providers (HCPs) and individuals with specific health problems followed the adoption of measures to prevent the spread of infections (HIV, Hepatitis) and bloodborne pathogens. It is estimated that more than 13 million people worldwide have a latex allergy.1
Data (2016) indicates that the average prevalence of latex allergy worldwide remains 9.7%, 7.2%, and 4.3% among healthcare providers, susceptible patients, and the general population, respectively.1
Investigations have shown that up to 17% of HCPs are sensitised to the allergenic proteins in latex and those at the highest risk of sensitisation include dental assistants, operating room personnel, hospital housekeeping and emergency medical technicians.2,3
What causes latex Allergies 1,4,5
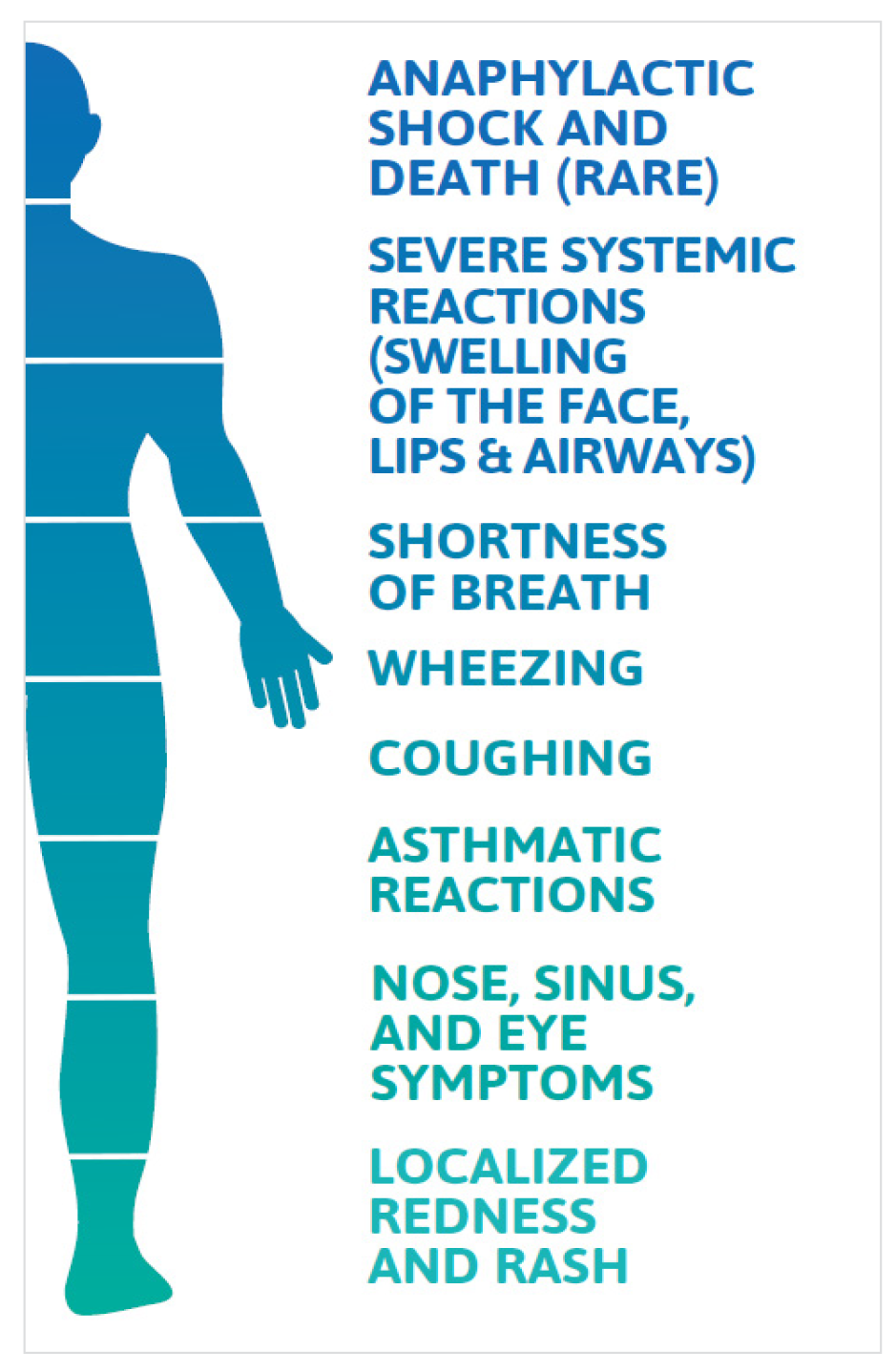
Latex allergy occurs when a person’s immune system reacts to certain proteins found in natural rubber latex (NRL). Of some 250 proteins in NRL, 15 have been identified as allergenic proteins that can elicit a hypersensitive immune response. Prolonged and repeated exposure to latex-allergenic proteins increases the risk and sensitisation to NRL (presence of latex specific e.g. antibodies) is a prerequisite to latex allergy. Latex-sensitive individuals are asymptomatic and generally unaware of their antibody status. Latex allergy occurs following latex exposure and is a systemic reaction leading to a range of reactions, as outlined in the infographic.
Exposure to NRL allergenic proteins occurs via mucous membranes, the vascular system, direct skin contact and inhalation. Inhalation occurs when the cornstarch inside powdered latex gloves binds to latex allergens and becomes airborne during the donning and doffing of gloves.

Population at risk of latex allergy5:
-
HCPs such as dentists, dental assistants, physicians, nurses, laboratory clinicians, medical technicians
-
Individuals with specific health problems including atopy (history of allergy)
-
Spina bifida
-
Myelodysplasia
-
Urogenital abnormalities
-
Multiple surgical interventions
-
Food allergies (bananas, kiwi, avocado, and chestnuts).
Prevalence of latex allergy among dental practitioners and patients
Healthcare workers including dentists and dental hygienists are the most affected occupational group for latex allergy due to their frequent donning and removal of latex gloves.1
Data shows that up to 17% of healthcare workers are sensitised to latex.2
Due to their frequent repeat exposure, all dental professionals who use latex gloves should be considered at high risk for allergic reactions.5
Even as many dental practices transition away from latex gloves, latex allergy remains a highly prevalent occupational health hazard among practitioners.
That is partly because latex is present not only in gloves but also in common dental products such as dental dams, bite blocks, mixing bowls, syringes, suction tips, oxygen masks, adhesive bandages and more.
The frequency with which dental practitioners contact additional latex products may not be as high as the exposure to allergens from a latex glove.
Management of latex allergy
Avoidance of latex is critical to managing latex allergy. Research shows that when measures were taken to minimise latex exposure during dental treatment, 81% of latex-allergic patients did not suffer adverse reactions.6
Additionally, management protocols for latex allergy are recommended, including steps to evaluate both staff and patients for their risk of latex allergy, guidelines to create a latex-safe environment, education about latex allergy and emergency preparedness for adverse patient or staff reactions, should they occur.7

Latex glove alternatives
Due to recent advancements in technology, nitrile gloves have significantly improved, making them a popular alternative to latex gloves in dental clinics.
These gloves are now more comfortable to wear, offer better grip, and have increased puncture and chemical resistance.
As a result, dental clinics may opt for nitrile gloves to provide better protection to their staff and patients.
For more information, please reach out to your Ansell or Henry Schein Representative.
Article Published Oct-Dec 2023 Dental Solutions
References
1. Wu M, McIntosh J, Liu J. Current prevalence rate of latex allergy: Why it remains a problem? J Occup Health. 58(2):138-144. March 2016
2. Dermata A, Arhakis A. Latex Allergy in Dental Care. Balk J Dent Med. Vol 18, 2014.
3. Burkhart C, Schloemer J, Zirwas M. Differentiation of Latex Allergy from Contact Dermatitis. Contact Dermatitis. Vol. 96, December 2015.
4. Pien L. Latex Allergy. Cleveland Clinic Centerfor Continuing Education. Disease Management. Published 2010. Reviewed 2017. http://www.clevelandclinicmeded.com/medicalpubs/ diseasemanagement/allergy/latex-allergy/
5. Katelaris C. Latex Allergy Diagnosis and Management. World Allergy Management. September 2016
6. Kean T, McNally M. Latex hypersensitivity: a closer look at considerations for dentistry. Journal of the Canadian Dental Association 2009
7. Hamann C, Rodgers P, Sullivan M. Prevalence of Type I Natural Rubber Latex Allergy Among Dental Hygienists. Journal of Dental Hygiene, Vol.79, No. 2, Spring 2005.